Knee Screening: Integrating Performance Training with Clinical Insight
Introduction: Why Knee Screening Is Critical
Why you should care?
Imagine if a comprehensive knee screening had been part of Derrick Rose’s development before and during his explosive rise in the NBA — could we have maybe seen one of the greatest players ever fully realize his potential? Football fans remember Ronaldo #9 (Ronaldo Luís Nazário de Lima), whose career was profoundly affected by knee injuries. In tennis, Pat Rafter had his prime repeatedly interrupted by persistent knee issues. Early identification of tendons, ligaments and neuromuscular risk factors might have prolonged their time at the top, or even elevated it further. Young talents like Nemanja Aleksandrov, once tipped as a future NBA first pick, never got a chance to play at that level due to debilitating knee injury. Even in the modern era, elite athletes continue to be affected: as recently as the 2026 Winter cycle, Lindsey Vonn suffered an ACL rupture just before Olympic competition, a stark reminder that without proper knee screening and early risk identification, even the best are vulnerable.
Although I’ve only mentioned a few high-profile professional athletes, the situation among young, developing athletes is even more striking. Statistics clearly show an enormous number of knee injuries arising from poor load management and flawed periodization. How can we implement effective load management and training periodization if we don’t first know the true condition of the athlete’s knee?
Knee injuries remain among the most common and performance-limiting injuries in sport, despite significant advances in surgical techniques, imaging, and rehabilitation protocols. For the strength and conditioning (S&C) coach, the knee represents a one of the most exposed joints to training load, neuromuscular control, and athletic performance, and it is the joint where training decisions most directly interact with injury risk.
strong>A good knee screening is not about diagnosing injuries—that’s the medical staff’s role—but it often highlights issues that require medical attention, and also allows the coach to detect subclinical problems, subtle dysfunctions that exist before symptoms appear. This information guides what you load, how you load it, and when you need to reduce or modify training. Proper screening enables smarter load management and individualized periodization, supporting athlete health, extending career longevity, and distinguishing expert coaches from general gym trainers.
At the very start of a knee screening protocol, the most basic and essential step is the assessment of passive structures, including ligaments and menisci. This initial evaluation provides a “green light” for safe progression to dynamic and performance-based testing, ensuring that subsequent assessments of muscular function, movement patterns, and load tolerance do not compromise structural integrity.
Screening should not stop at passive structures; in addition to evaluating ligaments and menisci, it must also assess muscular strength, rate and timing of activation, fatigue resistance, and the neuromuscular interaction between muscles and passive knee structures. Ligaments such as the ACL not only provide passive knee stability but also have a critical, often overlooked role as sensory organs, relaying joint position and tension information that triggers protective muscular responses. When this proprioceptive system is impaired and not evaluated, athletes may unknowingly train and compete with an elevated risk of knee injury.
Screening should also incorporate assessment of patellar tracking, early degenerative changes, and patellar tendon load tolerance. These factors are particularly relevant in jumping- and sprint-based sports but are still rarely evaluated in a structured manner by S&C practitioners. Subtle signs such as chondromalacia, patellar maltracking, or instability (e.g., positive J sign) may not yet produce pain or functional limitations, yet they can increase long-term injury risk and compromise performance if left unrecognized.
A comprehensive knee screening protocol therefore functions as risk mapping, identifying deficits across multiple layers—passive structural integrity (ligaments and menisci), muscular strength, RFD, and endurance, proprioception and neuromuscular control, as well as subtle or pre-symptomatic issues such as early chondromalacia and patellar maltracking (e.g., indicated by a positive J sign). This approach allows the S&C coach to individualize training, manage load intelligently, and collaborate effectively with medical teams. Screening is not diagnosis; it is a proactive framework that protects athletes today and preserves knee function for the future.
The Knee: Stability Under Load, Vulnerable to Chaos
From a biomechanical standpoint, the knee is a modified hinge joint designed primarily for flexion and extension, with a limited but highly regulated capacity for rotation. Stability requirements at the knee are extreme, and the joint has low tolerance for uncontrolled movement, especially under high velocity and external load. Functional knee stability in athletic environments depends on the precise interaction between passive restraints, active muscular control, and neuromuscular coordination during dynamic, sport-specific tasks.
Passive Structures
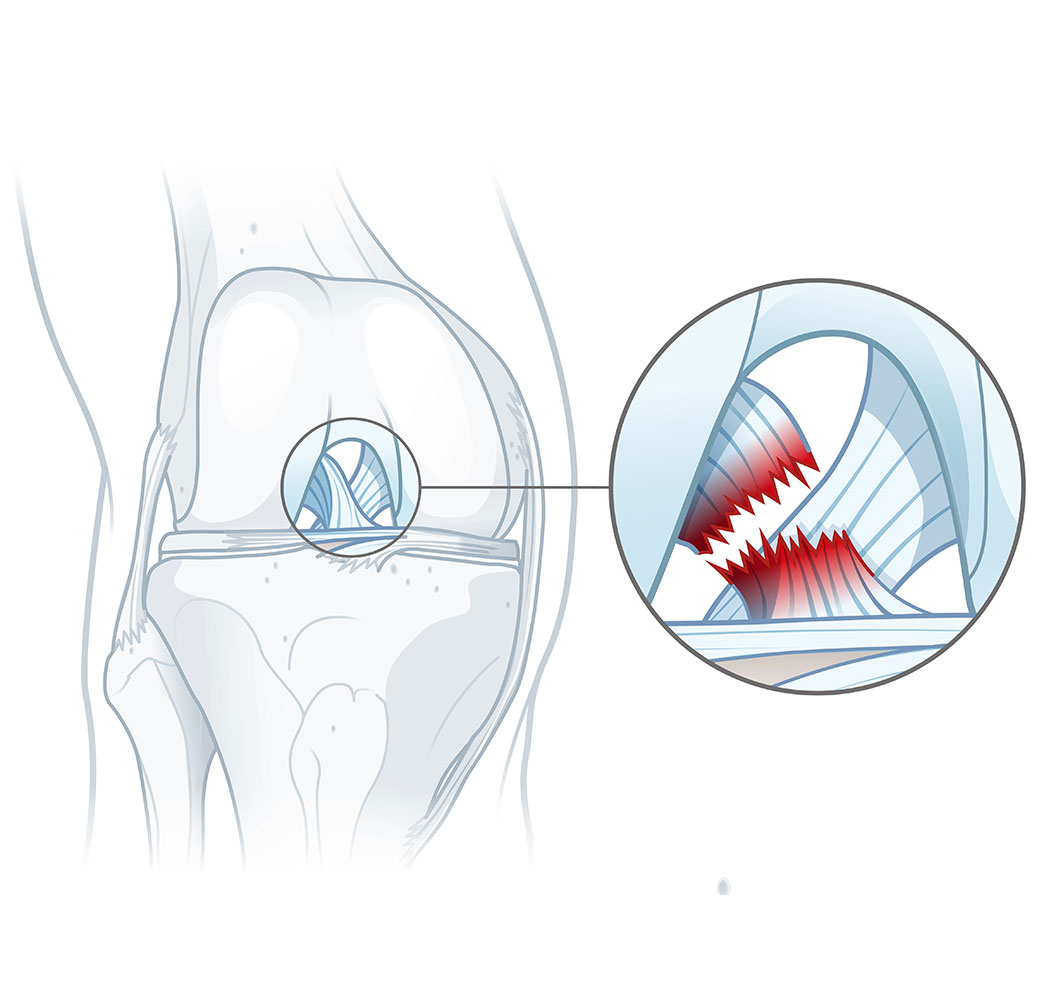
The Anterior Cruciate Ligament (ACL) prevents the tibia from sliding forward relative to the femur during high-demand actions such as sudden deceleration, cutting, or landing, when strong quadriceps contraction, ground reaction forces, valgus collapse, and internal tibial rotation act simultaneously on the knee. In these moments, the tibia is driven anteriorly and rotationally under the femur, and the ACL is the primary passive structure resisting this motion. Functionally, the ligament is most stressed during non-contact pivoting tasks, which explains the high incidence of ACL injuries across sports. In the United States alone, an estimated 200,000–250,000 ACL injuries occur annually, with over 130,000 reconstructions performed each year, particularly in collegiate and professional athletes. In Europe, incidence rates are comparable, with surgical and rehabilitation costs ranging from approximately €15,000–30,000 per athlete, while in the U.S. total costs often exceed $25,000–50,000 when surgery, rehabilitation, and time loss are included. Following reconstruction, return-to-competition typically occurs between 6 and 12 months, depending on graft type, concomitant injuries, rehabilitation adherence, and sport-specific demands. Despite surgical advances, 20–40% of athletes fail to return to their pre-injury performance level, highlighting that ACL injury is not merely a structural problem—it is a neuromechanical and performance problem. High-profile cases such as Derrick Rose, alongside numerous elite football, basketball, and skiing athletes (e.g., Lindsey Vonn), demonstrate that even after successful reconstruction, deficits in neuromuscular control, confidence, and movement efficiency can permanently limit athletic performance.
The Posterior Cruciate Ligament (PCL) limits posterior displacement of the tibia relative to the femur, particularly at higher degrees of knee flexion, by counteracting posterior shear forces generated during axial loading and quadriceps–hamstring co-contraction. Its role becomes dominant when bony congruency and capsular restraints are reduced, such as during falls onto a flexed knee or sudden deceleration with the knee deeply flexed. In sports like soccer, rugby, and alpine skiing, isolated PCL injuries are rare, accounting for approximately 3,000–10,000 cases annually in the United States, far fewer than ACL injuries. Typical mechanisms include direct impact to the anterior tibia during a tackle or collision, landing awkwardly on a flexed knee, or slipping and falling with the tibia driven posteriorly, such as sliding tackles in soccer or crashes in skiing. Because these injuries are uncommon, many surgeons have limited experience performing PCL reconstructions, and many rehabilitation specialists are unsure how to structure an optimal recovery program, making these injuries particularly challenging when they do occur. Treatment costs in Europe, including surgery and rehabilitation, typically range from €10,000–25,000, while in the U.S. total costs can reach $20,000–40,000. Recovery is generally slower than ACL reconstruction, with return to competition often delayed 9–12 months, and some athletes never fully regain pre-injury performance levels due to persistent posterior laxity or altered neuromuscular control.
The Medial Collateral Ligament (MCL) resists valgus stress and helps control external tibial rotation, particularly during early to mid-range knee flexion. Functionally, it works synergistically with the medial meniscus and hip abductors to maintain frontal plane stability. MCL injuries are relatively common in contact and cutting sports such as soccer, rugby, and American football, often resulting from direct lateral blows to the knee or valgus collapse during rapid change-of-direction movements. In total, MCL injuries affect an estimated 100,000–150,000 athletes annually in the U.S., of which 40,000–60,000 are isolated tears; the remainder occur in combination with ACL or other ligament injuries. MCL injuries rarely require surgical reconstruction, as most heal successfully with conservative management, while different grades of injury (I–III) determine recovery timelines:
- Grade I (Mild): A few days to 2–4 weeks for return to play; primarily conservative care including physiotherapy and bracing; costs in the U.S. typically $500–1,500, in Europe €400–1,200.
- Grade II (Moderate): 1–3 months, with change-of-direction sports potentially requiring 4–6+ months; treatment may include longer physiotherapy, functional bracing, occasional minor procedures; costs $1,500–5,000 (U.S.), €1,200–4,000 (Europe).
- Grade III (Severe/Complete): 3–6 months or more, often requiring a brace and structured rehab, sometimes 9+ months with surgery; combined surgical and rehabilitation costs range $10,000–25,000 (U.S.) and €8,000–20,000 (Europe).
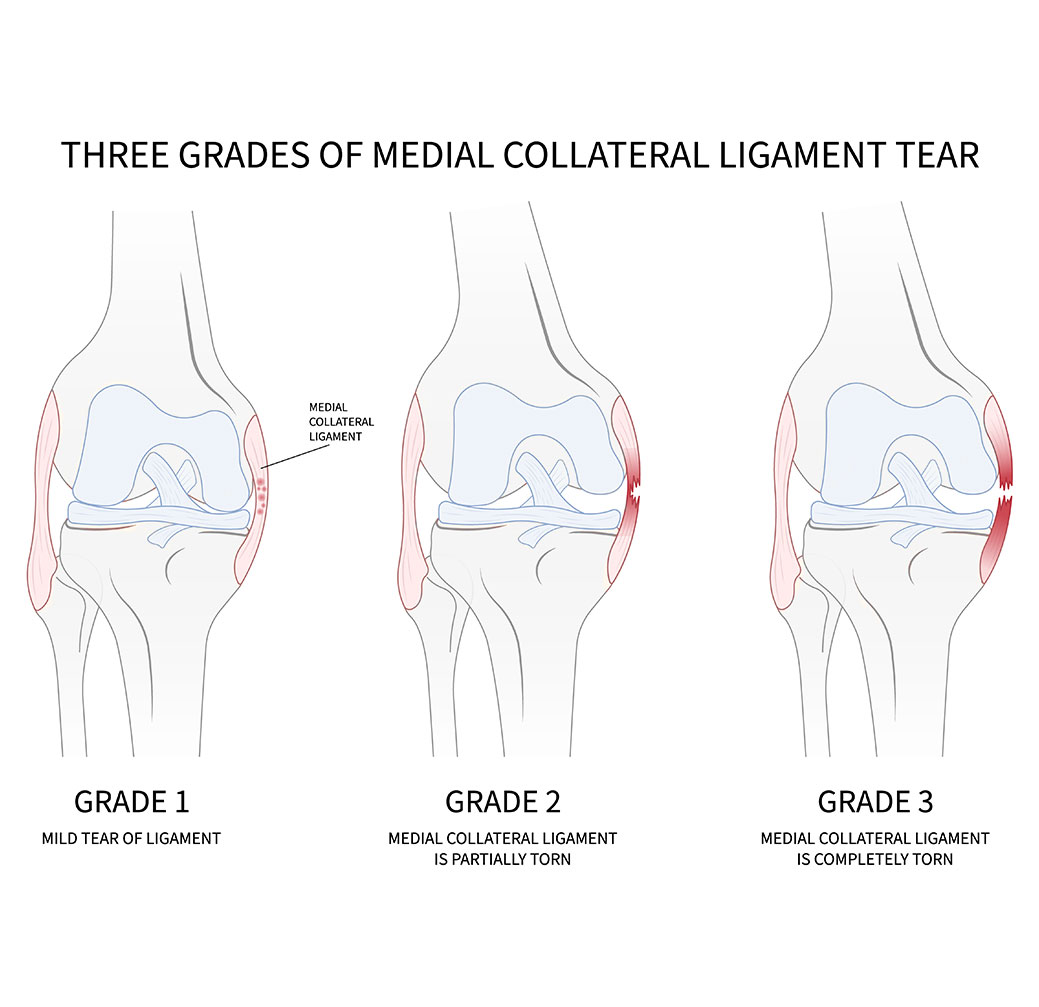
Athletes may still experience subtle medial instability or functional limitations even after apparent structural healing, particularly in combination injuries.
The Lateral Collateral Ligament (LCL) resists varus stress and contributes to posterolateral knee stability, particularly during mid- to high-range knee flexion. Isolated LCL injuries are rare, accounting for roughly 5,000–8,000 cases annually in the U.S., and usually occur during high-speed lateral cutting, awkward landings, or varus stress from collisions, as seen in ice hockey, American football, and skiing. Most LCL injuries occur in combination with ACL or PCL tears, providing clinicians with sufficient overall experience despite the rarity of isolated cases. Surgical reconstruction is rarely required, as most LCL injuries heal with conservative management including bracing and structured rehabilitation. Recovery varies by severity:
- Grade I (Mild sprain): 2–4 weeks; conservative care including physiotherapy and bracing; costs $500–1,500 (U.S.), €400–1,200 (Europe).
- Grade II (Partial tear): 4–8 weeks; more intensive physiotherapy, functional bracing; costs $1,500–4,000 (U.S.), €1,200–3,500 (Europe).
- Grade III (Complete tear): 8–12 weeks, sometimes longer if combined with other ligament injuries; costs $8,000–20,000 (U.S.), €6,000–15,000 (Europe).
Athletes may experience subtle posterolateral instability or functional limitations even after apparent structural healing, which can influence cutting, pivoting, and deceleration mechanics.
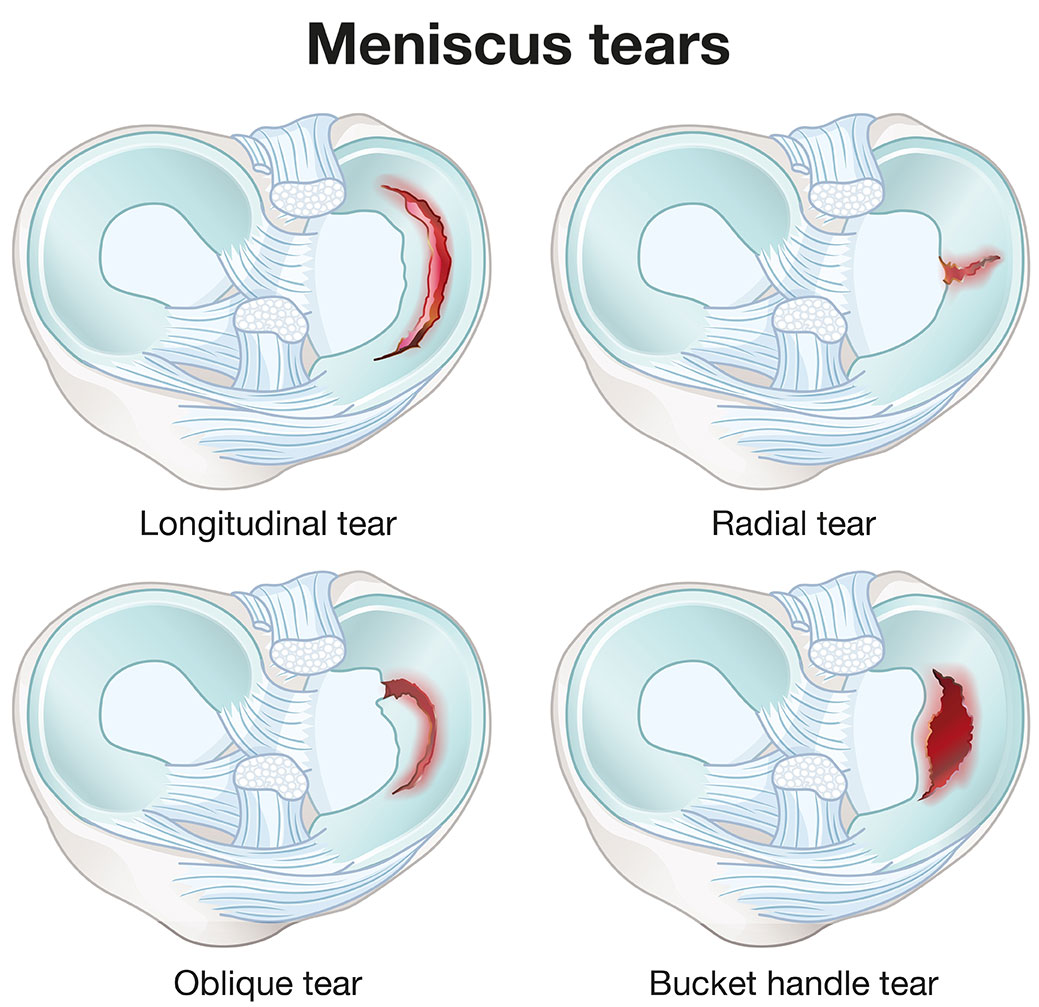
Menisci (Medial and Lateral) are the main shock absorbers of the knee, along with multiple other critical functions, including increasing tibiofemoral congruency, distributing compressive loads, assisting in joint lubrication, and providing secondary restraint to rotation, particularly in ACL-deficient knees. Meniscal injuries are common in sports involving cutting, pivoting, or contact, such as soccer, basketball, rugby, and skiing. In the U.S., approximately 150,000–200,000 meniscal injuries are diagnosed annually, with 40–60% occurring in combination with ACL tears, while isolated tears account for roughly 60,000–80,000 cases. In Europe, incidence is similar, with costs of treatment—including arthroscopy, physiotherapy, and post-operative care—ranging from €5,000–15,000 for isolated injuries, and up to €20,000–30,000 when combined with ligament reconstruction; in the U.S., total costs can reach $15,000–35,000, depending on surgery and rehabilitation.
Meniscal tears are classified based on morphology, location, and depth, with some variation between radiologic (MRI) and intraoperative classifications. Most scientific literature emphasizes tear patterns (radial, horizontal, longitudinal, bucket-handle, flap, complex) and location (medial/lateral, anterior/posterior horn), rather than a strict numeric grade. The Grade I–IV system used below is simplified for coaching and practical understanding, particularly to guide S&C decision-making and recovery expectations. Acute traumatic tears in athletes may not always fit neatly into traditional grading systems, and complex or combined tears are frequently associated with ligament injuries, which can influence both treatment and prognosis.
Meniscal Tear Classification:
- Grade I–II / Minor tears or degeneration: Small radial, horizontal, or oblique changes; often asymptomatic and typically managed conservatively. Commonly seen in early degenerative changes rather than acute trauma.
- Grade III / Full-thickness or complex tears: Includes longitudinal, bucket-handle, flap, or complex patterns; may require surgical intervention such as meniscus repair or partial meniscectomy. Full-thickness tears involve disruption through the entire meniscal depth.
- Grade IV / Extensive or combined tears: Usually associated with concomitant ligament injuries (ACL, PCL) or complex degenerative patterns; carries higher risk for long-term osteoarthritis. This grade is less commonly used in standard radiologic reporting but may be applied intraoperatively.
Recovery Timeline by Type:
- Conservative management / minor tears: 2–6 weeks, depending on symptoms and load tolerance.
- Partial meniscectomy: 4–8 weeks; athletes often return earlier for low-demand activities.
- Meniscus repair / complex tears: 3–6 months, sometimes longer if combined with ligament reconstruction, with cautious progression to cutting and pivoting sports.
Note: Recovery timelines are approximate and depend on tear location (vascular vs. avascular zone), patient age, concomitant injuries, and rehabilitation adherence.
While coaches and athletes often prioritize ACL over meniscus, long-term joint health depends heavily on meniscal integrity. Even if performance during the athlete’s career is maintained, meniscal damage greatly increases the risk of early-onset osteoarthritis, leaving former athletes with chronic pain, swelling, and functional limitation later in life. Proper recognition and structured rehabilitation of meniscal injuries are therefore essential both for immediate sports performance and long-term knee health.
Active Structures
Active muscular support plays a critical role in dynamic knee stability. The quadriceps are primary force generators for knee extension but also increase anterior tibial shear forces near terminal extension, potentially stressing the ACL in poorly controlled movement patterns. The hamstrings act as dynamic synergists to the ACL by producing posterior tibial shear; delayed or insufficient hamstring activation is a well-documented contributor to functional knee instability. The gastrocnemius and popliteus contribute to knee stabilization during dynamic tasks by assisting in rotational control, particularly during cutting, landing, and rapid deceleration.
Closely linked to quadriceps function, the patellar tendon serves as the primary force-transmission structure between the quadriceps and the tibia, playing a critical role in jumping, sprinting, and deceleration mechanics. Tendinopathic changes—common in volleyball, basketball, athletics, and football—do not primarily reflect a loss of strength, but impaired load tolerance and force transfer capacity. Athletes with patellar tendinopathy may demonstrate preserved maximal strength yet fail under repetitive or high-rate loading, increasing injury risk and reducing performance despite “normal” strength testing.
Closely linked to quadriceps function, the patellar tendon (patellar ligament) serves as the primary force-transmission structure between the quadriceps and the tibia, enabling knee extension during jumping, sprinting, cutting, and deceleration. Biomechanically, it is exposed to extremely high tensile loads, particularly during eccentric quadriceps action in landing and change-of-direction tasks, where force magnitude, loading rate, and repetition frequency converge. Tendinopathic changes—common in volleyball, basketball, athletics, and football—do not primarily reflect a loss of maximal strength, but impaired load tolerance and force transfer capacity. Athletes with patellar tendinopathy may demonstrate preserved maximal strength yet fail under repetitive or high-rate loading, increasing injury risk and reducing performance despite “normal” strength testing. Unlike ligament injuries, patellar tendon pathology most commonly develops as a chronic overload condition rather than an acute rupture, making it a quintessential load-management and screening problem.
Screening Considerations: Given its critical role in force transmission and susceptibility to chronic overload, structured knee screening should include assessment of patellar tendon load tolerance, particularly in athletes exposed to frequent jumping, sprinting, and cutting. Evaluating tendon response under controlled high-rate or repetitive loading can reveal subclinical deficits that are not apparent in maximal strength testing alone, allowing S&C practitioners to tailor load management and preventive interventions before symptomatic tendinopathy develops.
Patellar Tendon (Patellar Ligament)
The patellar tendon serves as the primary force-transmission structure between the quadriceps muscle group and the tibia, enabling knee extension during jumping, sprinting, cutting, and deceleration. Biomechanically, it is exposed to extremely high tensile loads, particularly during eccentric quadriceps action in landing and change-of-direction tasks. Unlike ligament injuries, patellar tendon pathology most commonly develops as a chronic overload condition rather than an acute rupture, making it a quintessential load-management and screening problem.
The patellar tendon serves as the primary force-transmission structure between the quadriceps muscle group and the tibia, enabling knee extension during jumping, sprinting, cutting, and deceleration. Biomechanically, it is exposed to extremely high tensile loads, particularly during eccentric quadriceps action in landing and change-of-direction tasks. Unlike ligament injuries, patellar tendon pathology most commonly develops as a chronic overload condition rather than an acute rupture, making it a quintessential load-management and screening problem.
Patellar tendon injuries are particularly prevalent in power- and jump-dominant sports. In elite volleyball and basketball players, 14–45% develop patellar tendon–related knee pain, corresponding to an estimated 2,000–6,000 cases annually in top-level professional and collegiate athletes in the U.S., with conservative management costs typically ranging from €3,000–8,000 in Europe and total treatment costs often exceeding $10,000–25,000 in the U.S., particularly when prolonged rehabilitation, missed training, and competition are included. Soccer players experience these injuries in roughly 10–20% of athletes, translating to 1,000–2,500 cases annually, while competitive track and field jumpers show similar prevalence. Across Europe and the U.S. combined, tens of thousands of athletes seek medical care for patellar tendon issues each year, with a substantial proportion progressing to chronic symptoms lasting six to twelve months or longer if improperly managed.
Classification of Patellar Tendon Injuries:
- Reactive / Early Tendinopathy: Load-related pain without structural disruption; performance often preserved but load tolerance reduced
- Degenerative Tendinopathy: Structural tendon changes, pain with sport-specific tasks, reduced force transmission efficiency
- Partial Tear: Focal disruption of tendon fibers, significant pain, and loss of explosive capacity
- Complete Rupture (Rare): Acute failure, usually in older or previously degenerated tendons; surgical repair required
Return to Sport and Recovery Timeline:
- Early-stage tendinopathy: 6–12 weeks with structured load modification and progressive rehabilitation
- Chronic degenerative tendinopathy: 3–9+ months, frequently with fluctuating symptoms
- Partial tears: 3–6 months, sometimes longer depending on load exposure
- Complete rupture: 6–12 months or more following surgical repair
Clinical Considerations:
Patellar tendon pathology is often underestimated in performance environments. Athletes may continue training despite symptoms, leading to tendon degeneration rather than resolution. Unlike many ligament injuries, degenerative tendon changes carry long-term consequences, including chronic knee pain, reduced function, and increased risk of early osteoarthritis. From both a performance and longevity perspective, patellar tendon health may be more critical than many acute ligament injuries, particularly in athletes competing in jump- and power-dominant sports.
Screening: Translating Structure and Function into Action
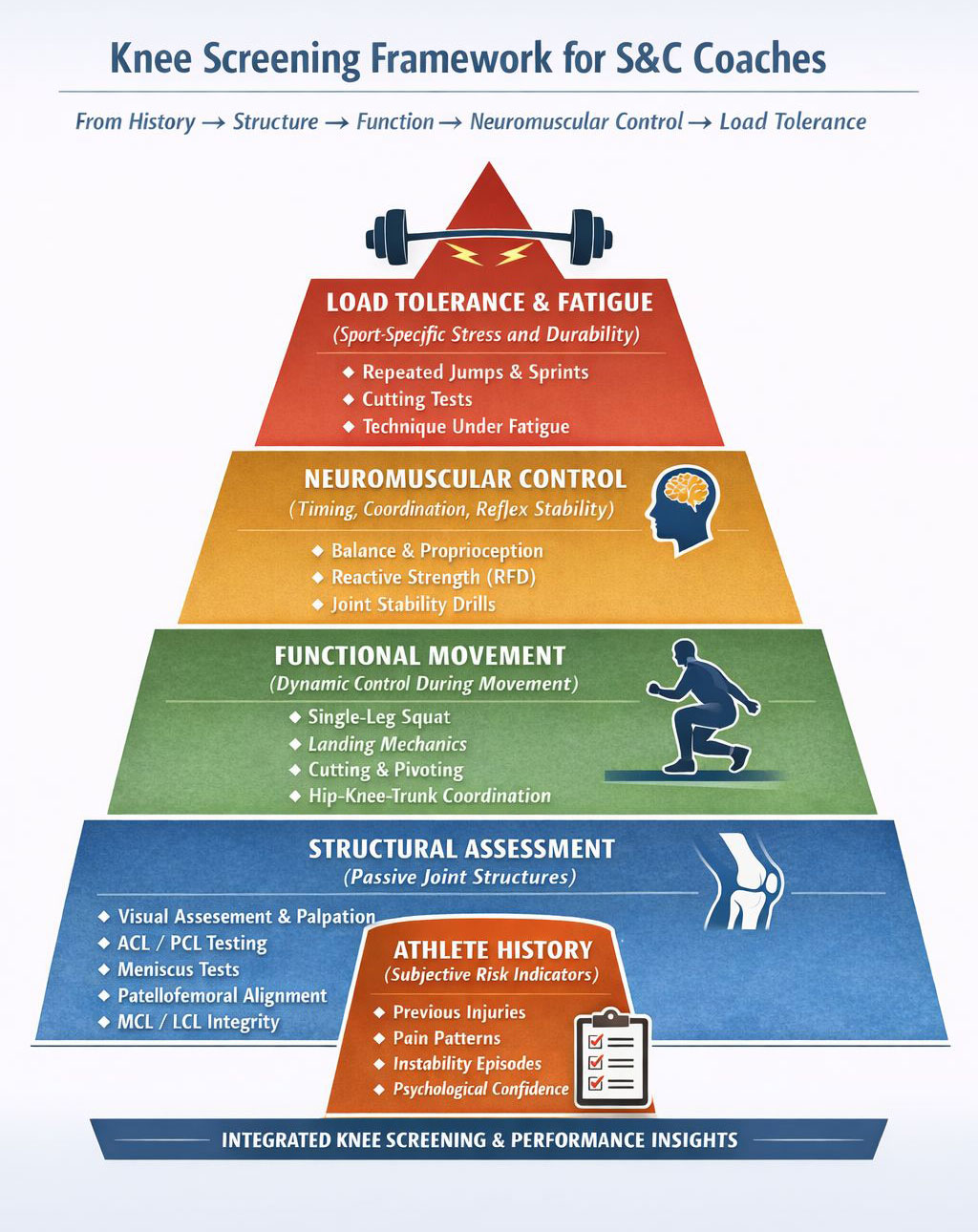
Effective knee screening identifies patterns of vulnerability rather than isolated findings. A comprehensive approach integrates multiple layers—subjective history, structural assessment, functional analysis, neuromuscular evaluation, and load tolerance testing—providing the S&C coach with a clear picture of knee behavior under both training and competitive conditions.
Following an introduction on key knee structures, injury prevalence, and the financial importance of adequate prevention, the next section presents an overview of essential knee screening tests. These assessments form the foundation for subsequent, more detailed discussions on evaluation and practical application in athletic settings.
Knee Screening: Structured Overview for S&C and Performance Teams
1. Subjective History and Athlete-Reported Symptoms
Before any objective testing, a detailed history identifies pre-existing risk factors:
- Previous injuries, surgeries, or instability episodes
- Pain location, timing, and activity triggers
- Episodes of giving way, locking, or swelling
- Psychological confidence and perceived knee control
Why it matters: An athlete who reports instability during deceleration or pivoting is already “screening positive,” highlighting areas that require further assessment even before clinical tests begin.
2. Structural and Clinical Assessment (Passive Structures)
Ligament Testing:
- Lachman Test: Gold standard for ACL integrity at 20–30° flexion
- Anterior Drawer Test: Secondary ACL assessment at 90° flexion
- Pivot Shift Test: Evaluates dynamic rotational instability
- Valgus/Varus Stress Tests: MCL/LCL integrity
Meniscal Evaluation:
- McMurray Test
- Thessaly Test
- Joint line palpation
Patellofemoral Assessment
- J-sign, patellar tracking, subtle malalignment
- Early chondromalacia evaluation
Why it matters: Detects passive structural vulnerabilities and predisposing factors for anterior knee pain or chronic injury, allowing safe progression to functional testing.
3. Functional Movement Analysis (Active Structures)
Observing movement patterns under controlled and sport-specific conditions provides insight into dynamic stability:
- Single-leg squat and step-down
- Drop landing and jump-landing mechanics
- Cutting, pivoting, acceleration, and deceleration drills
- Trunk-knee-hip coordination in frontal and transverse planes
- Observing fatigue effects on movement quality
Goal: Identify dynamic valgus/varus tendencies, asymmetries, delayed muscle activation, and compensatory strategies that increase ligament, meniscus, or patellar tendon strain.
4. Neuromuscular and Proprioceptive Assessment
- Balance and postural control: single-leg stance, wobble boards, Bosu, stabilometry
- Reactive strength and rate of force development (RFD), particularly hamstrings and quadriceps
- Dynamic joint position sense and perturbation response: evaluates timing and quality of corrective muscular responses
Why it matters: Strength alone is not protective. Muscles must contract rapidly, in proper sequence, and at the right amplitude to stabilize the knee. Delayed or weak activation under high load increases ACL, meniscus, and patellar tendon injury risk. This assessment identifies neuromuscular deficits not apparent in isolated strength or power testing.
5. Load Tolerance and Fatigue Assessment
- Repeated sprint or jump protocols simulating sport-specific fatigue
- Monitoring technique degradation and compensatory strategies under load
- High-intensity deceleration and cutting tasks to reveal vulnerability under real conditions
Goal: Understand how fatigue and repeated stress affect knee stability, allowing coaches to individualize training loads and progression safely.
6. Instrumented Tools for Muscle Function, Force, Power, and Neuromuscular Control
- Isokinetic Dynamometry: Measures peak torque, RFD, and muscular endurance; detects asymmetries not apparent in manual testing; useful in post-ACL, PCL, or meniscus rehab.
- Force Plates / Pressure Sensors: Quantify ground reaction forces, landing symmetry, and load distribution; reveal compensatory strategies under dynamic conditions.
- Electromyography (EMG / eEMG): Measures muscle activation patterns, timing, and co-contraction of hamstrings, quadriceps, gastrocnemius, and gluteals; when combined with motion capture, allows precise mapping of neuromuscular strategies.
Integration in Knee Screening:
These tools are complementary to clinical and functional assessments. Objective measurements allow coaches and rehab specialists to quantify deficits, monitor recovery, and individualize training. In elite sport, EMG and force/pressure data can predict ACL load, optimize landing mechanics, and reduce injury risk.
Key Takeaways
- Screening maps risk, it does not grant clearance. It identifies vulnerabilities starting with passive structures(ligaments, menisci, patellofemoral alignment), progressing to active and muscular function (strength, coordination, tendon load tolerance), and culminating in neuromuscular control and fatigue response.
- Functional deficits may be hidden. Athletes can appear structurally sound yet exhibit high-risk movement patterns or impaired load tolerance under sport-specific conditions, which only become evident through integrated assessment.
- Integration drives decisions. Combining information from athlete history, structural evaluation, movement observation, muscle performance, and instrumented measures allows for individualized training, load management, injury prevention, and informed return-to-sport planning.
- Long-term joint health is critical. Even subtle deficits in meniscus, patellofemoral tracking, or tendon function may have minimal short-term impact on performance but are major determinants of lifelong knee integrity and injury risk.
Conclusion
Knee screening is not just a test—it is your only window into potential subclinical deficits and risk factors that might threaten performance and career longevity. Without a structured, multi-layered assessment of ligaments, menisci, patellar tendon, muscular abilities, and neuromuscular function, your training program operates in the dark and represents a form of guessing. Screening is the S&C coach’s tool for intelligent load management, injury prevention, and optimized athlete performance.
In the next article, we move from theory to structured practice. The step most often overlooked in knee assessment — athlete profiling — starts with a guided interview and a tailored questionnaire. The interview is not small talk; it is a purposeful conversation built around targeted questions. Through this intake, we collect information on injury history, swelling, instability, load intolerance, and mechanical symptoms. Key concerns may reveal red flags even before testing begins. A well-designed questionnaire strengthens professionalism, provides legal protection, and allows monitoring of subjective experiences that cannot be measured directly, such as pain, giving-way sensations, or stiffness. Documented progress is essential for performance decisions and long-term business development. Without understanding an athlete’s exposure and load-response patterns, no screening protocol — however advanced — can yield reliable insights. Assessment does not begin with movement; it begins with the right questions.
Table Of Contents
Part I – Why the Knee Fails
Explores why knee injuries are common and often non‑contact, driven by poor load management and misunderstood tissue capacity.
Why it matters: Understanding epidemiology and load patterns helps prevent predictable injuries before they occur.
Example: Derrick Rose’s repeated ACL setbacks highlight how unmanaged load and movement demands can curtail elite performance.
Part II – Athlete Profiling Before Physical Testing
Introduces structured intake through interview and tailored questionnaire before any physical testing.
Why it matters: Profiling reveals history, pain behavior, and load responses that inform safe, personalized training plans.
Example: Athletes who report instability or swelling in intake often show patterns linked to future knee issues, enabling early intervention.
Part III – Visual Estimation (Global and Segmental)
Assesses posture and movement patterns (static and dynamic) to identify risky mechanics.
Why it matters: Early observation of alignment or compensations predicts how the knee will handle sport demands.
Example: Women’s soccer teams reduced ACL patterns after identifying valgus collapse and trunk compensation in cutting drills.
Part IV – Palpation and Local Tissue Identification
Uses touch to identify painful structures such as tendons, bursae, and joint lines.
Why it matters: Palpation detects inflammation and localized pain that performance metrics alone miss.
Example: Early detection of infrapatellar bursitis in basketball prevented chronic flare‑ups and guided training modifications.
Part V – Patellofemoral Joint and Chondromalacia
Focuses on anterior knee pain and patellar mechanics, including tracking and cartilage stress signs.
Why it matters: Identifying patellar stress patterns avoids exacerbation through inappropriate loading.
Example: Volleyball athletes improved knee comfort when tracking deficits were corrected with targeted hip and quad work.
Part VI – Passive Structure Screening
Tests ligaments and meniscus integrity (e.g., Lachman, drawer tests, McMurray, Thessaly).
Why it matters: Ensures structural safety before advancing to higher loads or dynamic testing.
Example: A collegiate soccer player’s undetected meniscus lesion later ruptured during drills; early screening may have guided safer progression.
Part VII – Functional and Neuromuscular Assessment
Evaluates neuromuscular control, symmetry, strength under load, RFD, and coordination.
Why it matters: True performance stability requires muscles to respond quickly and correctly under sport‑specific stress.
Example: Programs using EMG timing feedback improved activation patterns and reduced non‑contact knee strain in contact sports.
Part VIII – Load Tolerance and Tissue Capacity
Assesses how tissues tolerate repeated and high‑intensity loads, fatigue, and progression stress.
Why it matters: Identifies safe workload limits and prevents chronic overload injuries.
Example: Without tendon load testing, athletes exposed to intense plyometrics developed chronic patellar tendinopathy, which structured load assessment might have prevented.
Part IX – Youth Athlete Considerations
Adapts knee assessment to growth‑related biomechanical changes and vulnerability in young athletes.
Why it matters: Growth spurts and immature coordination can create hidden risks if periodization isn’t adjusted.
Example: Rapidly growing youth soccer players showed deteriorating landing mechanics and knee discomfort until loads were tailored to developmental status.
Part X – Integrated Decision‑Making Model
Synthesizes all assessment layers into a risk profiling system with clear criteria for monitoring, modifying, and referring.
Why it matters: Converts assessment data into actionable training decisions to manage risk and performance.
Example: Performance teams using integrated risk categories (Green/Yellow/Red) consistently reported fewer knee injuries across a season compared to isolated testing approaches.









Responses