Visual Knee Estimation (Global and Segmental)
Seeing Before Touching: The First Layer of Objective Observation
Visual estimation represents the first objective step in the structured knee screening process, following athlete profiling through interview and questionnaire. Before any palpation, manual examination, or physical testing, systematic observation already provides relevant information about how the athlete presents in both static and dynamic conditions. In this sense, visual estimation bridges subjective reporting and subsequent objective assessment.
In high-performance environments, where time constraints are substantial and athletes may present without overt symptoms despite functional deficits or underlying morphological variations, visual estimation becomes a critical filtering mechanism in the decision-making process.
It is important to emphasize that visual estimation extends beyond movement observation during training or performance tasks and represents a fundamental element of the assessment process that precedes any palpation, manual examination, or hands-on testing. Through systematic observation of the athlete in a static and unloaded state, practitioners can identify relevant postural characteristics, asymmetries, alignment patterns, and morphological features before physical contact is established.
Consequently, visual estimation serves as a critical preliminary stage within knee screening and performance assessment, rather than merely an adjunct component.
Its role is not to establish a diagnosis—this lies outside the scope of strength and conditioning practice and, in many cases, beyond the primary responsibility of performance staff—but to identify observable patterns that may indicate swelling (effusion), local inflammatory signs, changes in skin coloration (erythema or discoloration), and alterations in tissue appearance such as increased glossiness or a “shiny” aspect, which may suggest fluid accumulation or an acute tissue response to load.
It may also reveal movement-related compensations, morphological adaptations associated with altered load distribution over time, and early signs of tissue overload. In cases where findings exceed the practitioner’s scope of competence, appropriate referral to a relevant healthcare or medical professional should be made.
In addition, visual assessment can provide valuable insight into chronic or recurrent conditions such as patellar tendon thickening consistent with patellar tendinopathy, persistent or exercise-induced joint effusion, and overuse-related changes commonly observed in conditions such as Osgood–Schlatter disease. Repeated post-exercise swelling patterns, when combined with information from athlete questionnaires discussed in the previous section, may further indicate inadequate load management or recovery deficits.
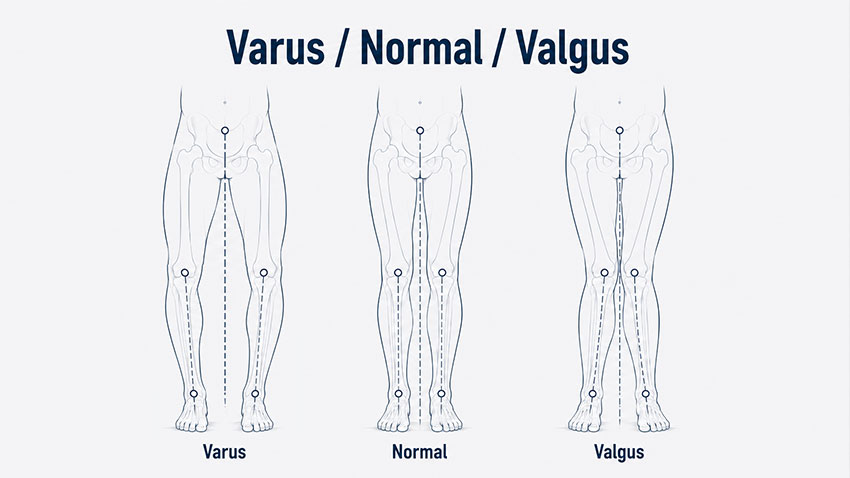
Furthermore, visual observation can highlight structural and biomechanical deviations such as genu valgum, genu varum, and genu recurvatum, as well as foot and ankle alignment issues that contribute to altered kinetic chain function and load transfer during movement.
Numerous examples from applied and research settings demonstrate that movement patterns are often preceded by identifiable static predispositions. While dynamic valgus collapse during landing is widely described in the literature as a multifactorial risk factor for anterior cruciate ligament injury—frequently associated with insufficient hip abductor function, particularly the gluteus medius—its foundation is often visible in static alignment characteristics such as femoral internal rotation tendency or frontal plane knee positioning. Similarly, rotational deviations observed during gait or stance may reflect underlying torsional alignment or neuromuscular organization that later manifests under dynamic loading. Although these examples are typically explored within dynamic assessment, their structural or postural precursors/consequences are frequently detectable in static conditions.
The purpose of visual estimation at the beginning of screening is therefore not to confirm presence/absence of pathology, but to detect deviations from expected biomechanical organization under controlled conditions, including both unloaded and low-load standing positions (when not limited by pain or injury). These deviations may represent long-term structural adaptations, compensatory movement strategies, or training-related responses to chronic loading.
Static and Dynamic Conditions
Visual estimation should be understood across two primary conditions: static and dynamic.
The static condition refers to observation of the athlete in non-moving positions such as standing or lying. The focus is on resting alignment, limb orientation, rotational tendencies, and visible asymmetries, reflecting baseline postural organization under minimal mechanical demand.
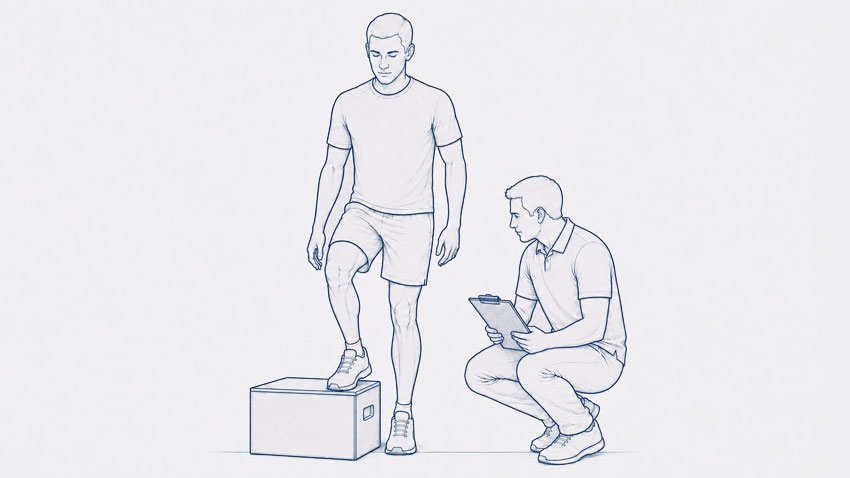
The dynamic condition refers to the athlete during movement, including locomotion, transitions, load acceptance, deceleration patterns, and task-specific motor solutions. Even basic walking and natural movement during approach to assessment can provide early insight into habitual motor behavior. When direct dynamic observation is limited due to injury, video material from training, competition, or the moment of injury may provide valuable additional information on movement strategies and compensations.
This distinction is essential, as certain deviations are already present at rest and serve as a structural or neuromuscular baseline for subsequent movement behavior, while others become apparent only under dynamic conditions and during exposure to load and activity.
Segmental and Global Assessment
Within both static and dynamic contexts, visual estimation can be organized into two complementary domains: segmental and global assessment.
Segmental assessment focuses on local knee-related features such as joint contour, muscle morphology, swelling patterns, and other tissue-level indicators that may reflect loading response, prior injury, or ongoing adaptation.
Global assessment, in contrast, evaluates overall posture, inter-segment alignment, and kinetic chain relationships. Deviations at the hip and knee, rotational alignment of the femur and tibia, and pelvic asymmetries may influence how load is distributed across the lower extremity. In elite sport, such patterns are frequently present, but their relevance depends on their interaction with sport-specific demands and cumulative load exposure.
When integrated, segmental and global observation form a rapid, non-invasive framework for initial risk stratification. This framework does not replace subsequent testing, but directly informs it by guiding the selection and sequencing of further assessment procedures.
In cases of injury, dynamic global observation may be limited depending on severity and stage, particularly in ACL injuries where certain motor tasks may not be feasible. In such situations, video analysis from training, competition, or the injury event itself can provide essential supplementary information that cannot be obtained in the clinical setting alone.
Static Knee Visual Estimation: Reading the System at Rest
Static visual estimation represents the first objective layer of observation within a controlled environment, where the athlete is evaluated in static positions such as unloaded (lying) and low-load standing, without externally imposed movement or task demands. Within the broader screening framework, it provides a foundational reference point against which all subsequent dynamic and load-based assessments are interpreted.
In the context of ACL injury, the applicability of static observation is influenced by cases where ACL injury may affect weight-bearing tolerance and standing assessment (particularly in the acute post-injury phase, immediately post-surgery, or in the presence of complications where standing may be limited or not feasible).
In lying positions, resting alignment and segmental organization allow observation of joint orientation, limb positioning, and soft tissue symmetry under minimal gravitational influence, providing a baseline reference for static assessment. In the case of standing, maintenance of posture requires continuous integration of gravitational forces, passive structural constraints, and neuromuscular control mechanisms. The resulting alignment and segmental organization therefore reflect a continuum shaped by structural alignment characteristics, adaptations to previous injury history, and responses to current diagnosed or undiagnosed conditions, as well as early indicators of reduced load tolerance that are not yet expressed as pain or performance limitation.
From a performance and injury-risk perspective, structural alignment observed under low-load conditions influences how forces will be distributed once external load, velocity, and task complexity are introduced. In this sense, static visual estimation does not merely describe posture—it defines the baseline mechanical framework within which all dynamic movement occurs.
It is important to emphasize that visual estimation operates across both global and segmental levels and within both static and dynamic contexts. However, comprehensive global analysis of the entire kinetic chain requires broader methodological depth than can be addressed within a single section.
For this reason, the present section is intentionally focused on segmental visual estimation of the knee joint under static conditions, including unloaded (lying) and standing positions. This approach allows for a detailed and structured analysis of knee-specific alignment, joint contour, and tissue-related indicators, which are directly relevant for subsequent stages of screening, including palpation, functional testing, and load tolerance assessment.
Visual estimation operates across both global and segmental levels and within both static and dynamic contexts. However, comprehensive global analysis of the entire kinetic chain requires broader methodological depth than can be addressed within a single section. For this reason, the present section focuses on segmental visual estimation of the knee under static conditions — both unloaded and standing — as a high-resolution local reference that can later be integrated with global and dynamic observations.
Frontal Plane Alignment: Varus and Valgus Organization
Rationale and Observational Framework
Frontal plane knee alignment represents a central component of segmental visual estimation, as it reflects both structural morphology and the distribution of load across the medial and lateral compartments of the tibiofemoral joint under different loading conditions. Within the structured screening sequence, assessment begins in non-weight-bearing conditions and progressively transitions toward weight-bearing observation, allowing separation of structural and functional contributors to alignment.
In non-weight-bearing positions (e.g., supine), frontal plane alignment primarily reflects structural or morphological organization of the limb, with minimal influence from axial loading, muscular co-contraction, or postural control demands. This provides a baseline reference for joint orientation and segmental alignment in the absence of external load.
As the assessment progresses toward standing (weight-bearing) conditions, alignment is evaluated under increasing postural demand, where passive structural characteristics interact with neuromuscular control strategies. This transition enables observation of how alignment is maintained or modified under load, and whether previously observed structural patterns are preserved, attenuated, or amplified.
Within this framework, non-weight-bearing and weight-bearing observations are not interpreted hierarchically as more or less valid, but rather as complementary conditions that provide different layers of information. Their combined use allows differentiation between:
- structural (morphological) deviations, which remain present regardless of loading condition
- functional (neuromuscular) deviations, which emerge or become more pronounced under weight-bearing conditions
This distinction is critical, as it directly influences both interpretation and subsequent intervention strategy.
Standardized Observation Procedure
To ensure consistency and reduce observational bias, the assessment follows a standardized protocol across both non-weight-bearing and weight-bearing conditions.
1. Non-weight-bearing (baseline position)
Athlete positioning (supine or equivalent relaxed position):
- Lower limbs fully relaxed without active muscular engagement
- Knee joints positioned in neutral extension without forced positioning
- No external correction of rotation or alignment
- Observation focused on resting frontal plane orientation of femur–tibia relationship
2. Weight-bearing (standing position)
Note: This assessment is not performed in cases where injury or clinical status precludes or contraindicates weight-bearing, in which case evaluation is limited to non-weight-bearing conditions.
Athlete positioning:
- Upright, relaxed stance
- Feet approximately hip-width apart
- Neutral foot progression angle (no forced external or internal rotation)
- Self-selected weight-bearing distribution between limbs (allowing natural asymmetries to be observed)
- Knees in extension without active hyperextension locking
Observer positioning:
- Primary observation from anterior view
- Secondary confirmation from posterior view
- Eye level aligned approximately with knee joint to minimize parallax error
- Elevated top-down perspective should be avoided, as it may distort frontal plane interpretation
- Level or slightly lower viewing angle provides the most accurate assessment of the hip–knee–ankle relationship
Key Visual Patterns in Knee Structure, Alignment and Tissue Response
Valgus Alignment: Functional and Structural Considerations
A valgus alignment pattern is characterized by medial displacement of the knee relative to the hip and foot. In athletic populations, this presentation is most commonly functional in origin, although structural contributors may also be present.
From a neuromuscular perspective, valgus alignment is frequently associated with:
- insufficient force production or delayed activation of the hip abductors (primarily gluteus medius)
- reduced contribution of hip external rotators
- quadriceps-dominant strategies with limited posterior chain involvement
These factors contribute to a characteristic kinetic chain configuration involving:
- hip adduction
- femoral internal rotation
- relative tibial external rotation
Even in static observation, this pattern may reflect an underlying motor strategy that becomes more pronounced under dynamic loading conditions such as landing, cutting, or deceleration.
Bidirectional Relationship: Cause and Adaptation
Valgus alignment operates within a bidirectional framework:
- Primary (driven by control deficits): neuromuscular insufficiency contributes to valgus positioning
- Secondary (adaptive response): persistent valgus positioning further alters motor recruitment and reinforces the pattern
This creates a self-sustaining interaction between alignment and neuromuscular control.
Mechanical Consequences and Injury Risk
From a load distribution perspective, valgus alignment increases:
- lateral compartment compressive stress
- medial structure tensile loading (including the MCL–meniscus complex)
This combined loading environment is particularly relevant in high-velocity tasks involving deceleration and change of direction.
A strong association may exist between dynamic valgus patterns and ACL injury mechanisms, especially in non-contact scenarios. When present even in static observation, valgus alignment should be considered a higher-priority screening finding rather than a neutral variation.
Additionally, valgus alignment is frequently accompanied by distal kinetic chain adaptations, including pes plano-valgus foot posture, which may further amplify medial collapse tendencies.
Varus Alignment: Structural Predisposition and Load Distribution
Varus alignment is characterized by lateral displacement of the knee relative to the hip and ankle, resulting in increased medial compartment loading.
In athletic populations, varus alignment is more commonly associated with structural factors such as:
- osseous alignment variations
- developmental morphology
- long-term skeletal adaptations
Functionally, this pattern leads to:
- increased medial tibiofemoral compressive stress
- reduced load-sharing capacity across the joint
Neuromuscular Interaction and Adaptation
Although often structurally driven, varus alignment interacts with neuromuscular control strategies. Over time, muscle activation patterns adapt to the existing alignment, which may reduce mechanical efficiency and alter force transmission.
As with valgus patterns, a bidirectional relationship exists between structure and function, where each influences and reinforces the other.
Mechanical Consequences and Long-Term Load Effects
The primary mechanical implication of varus alignment is chronic medial compartment overload, which might be associated with:
- medial meniscus degeneration
- articular cartilage stress accumulation
- progressive joint loading imbalance
Unlike valgus alignment, varus patterns are less directly linked to acute ligamentous injury but represent a relevant long-term degenerative risk profile under repeated loading.
Sagittal Plane Consideration: Genu Recurvatum
Observation Procedure
Assessment of sagittal plane knee alignment should be performed under both non-weight-bearing (lying) and weight-bearing (standing) conditions.
Non-weight-bearing assessment
- Athlete positioned in lying with both heels supported on an elevated surface
- No support should be placed beneath the knees
- The knees are allowed to assume their natural terminal extension position under the influence of gravity
- Observation should focus on the degree of terminal knee extension (or hyperextension) present in each limb, followed by side-to-side comparison to identify potential asymmetries
Weight-bearing assessment
- Athlete positioned in a relaxed standing posture
- Knees maintained in their natural position without intentional correction
- Observation performed under normal weight-bearing conditions when clinically appropriate
Observer positioning
- Primary observation from the lateral view
- Eye level aligned approximately with the knee joint to minimize visual distortion
- Side-to-side comparison is recommended under both non-weight-bearing and standing conditions
Comparison between non-weight-bearing and weight-bearing observations may assist in differentiating structural extension characteristics from patterns that become more evident under the influence of postural control and weight-bearing demands.
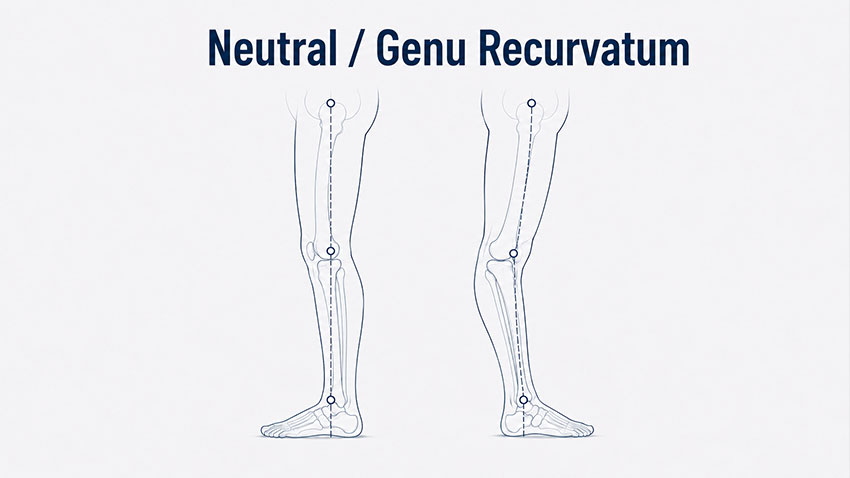
Genu Recurvatum
Genu recurvatum (knee hyperextension) is characterized by posterior displacement of the tibia relative to the femur beyond neutral extension. A small degree of hyperextension is considered a normal anatomical finding in many healthy individuals and athletes, typically ranging between approximately 0° and 5°, although greater values may be observed depending on age, sex, joint morphology, and generalized ligamentous laxity. The clinical relevance therefore lies not only in the absolute amount of hyperextension, but also in side-to-side symmetry and the athlete's injury history.
This pattern may be:
- structural (ligamentous laxity or joint morphology)
- functional (motor control strategy, quadriceps dominance, reduced hamstring contribution)
Mechanically, it alters:
- joint loading distribution
- ligamentous tension patterns
- neuromuscular timing during stance and movement
Excessive reliance on passive stabilization in terminal extension may reduce active muscular contribution, increasing vulnerability under dynamic load.
From a screening perspective, observation of terminal knee extension is particularly important because the objective is not only to identify excessive hyperextension, but also to determine whether symmetrical extension is present between limbs. This is especially relevant in athletes with current or previous knee injuries, where even small side-to-side differences may have functional significance.
In the context of ACL injury management, restoration of symmetrical terminal extension is considered a critical objective during both preoperative and postoperative rehabilitation. Before ACL reconstruction, achieving full extension comparable to the contralateral limb is widely regarded as a prerequisite for optimal surgical outcomes. Following surgery, restoration of full and symmetrical extension is typically expected during the early rehabilitation period, as persistent extension deficits are associated with altered gait mechanics and a higher risk of long-term functional limitations.
Failure to restore full extension may impair normal heel-strike during gait and lead to compensatory movement strategies. In more pronounced cases, athletes may demonstrate a persistent gait asymmetry or inability to achieve efficient running and sprinting mechanics. For this reason, visual observation of walking patterns, whenever not limited by injury status, represents a valuable complementary component of knee screening, as extension deficits often become apparent during locomotion before they are identified through formal testing.
Similar considerations apply to certain meniscal injuries, particularly displaced bucket-handle tears, which may mechanically block knee motion. Depending on the size and position of the displaced fragment, the knee may become effectively "locked" in a flexed position, resulting in a characteristic extension deficit that can substantially influence treatment strategy and surgical decision-making.
Persistence of hyperextension or extension asymmetry across both non-weight-bearing and standing conditions may suggest a stronger structural component, whereas differences that become more apparent during standing may indicate a greater contribution of postural control and neuromuscular factors.
Q-Angle Estimation and Patellofemoral Alignment
Rationale and Observational Framework
Within frontal plane assessment, estimation of the Q-angle provides insight into patellofemoral alignment and the resultant direction of force transmission through the anterior knee. Although precise quantification requires goniometric or imaging-based methods, visual estimation is sufficient in screening contexts to identify relevant deviations, asymmetries, and consistent alignment patterns.








Responses