Tapering Physiology
Introduction
The goal of any elite athlete or coach is to maximise the training adaptations in order to achieve pinnacle performance during competition (Grivas, 2018; Le Meur, Hausswirth and Mujika, 2012; Tonnessen et al., 2014). This involves the intricate, fluid and progressive planning of temporary and permanent training variables and performance goals to elicit the positive adaptations in response to period of progressive overload, supplemented by periods of restoration with the goal of supercompensation (Norris and Smith, 2002; Bompa and Haff, 2009; Haff and Triplett, 2015; Kiely, 2018; Mujika et al., 2018). These strategic periods of restoration are defined as tapers (Le Meur, Hausswirth and Mujika, 2012; Bosquet et al., 2007), which are brief periods of reduced training load with the maintenance of training intensity before a planned performance with the aim of improving performance (Bosquet et al., 2007) by dissipating the preceding accumulated fatigue and allowing supercompensation and adaptation (Mujika and Padilla, 2003; Plisk and Stone, 2003), with the greater the preceding accumulated fatigue, the greater reduction in training load necessary (Wilson and Wilson, 2008).
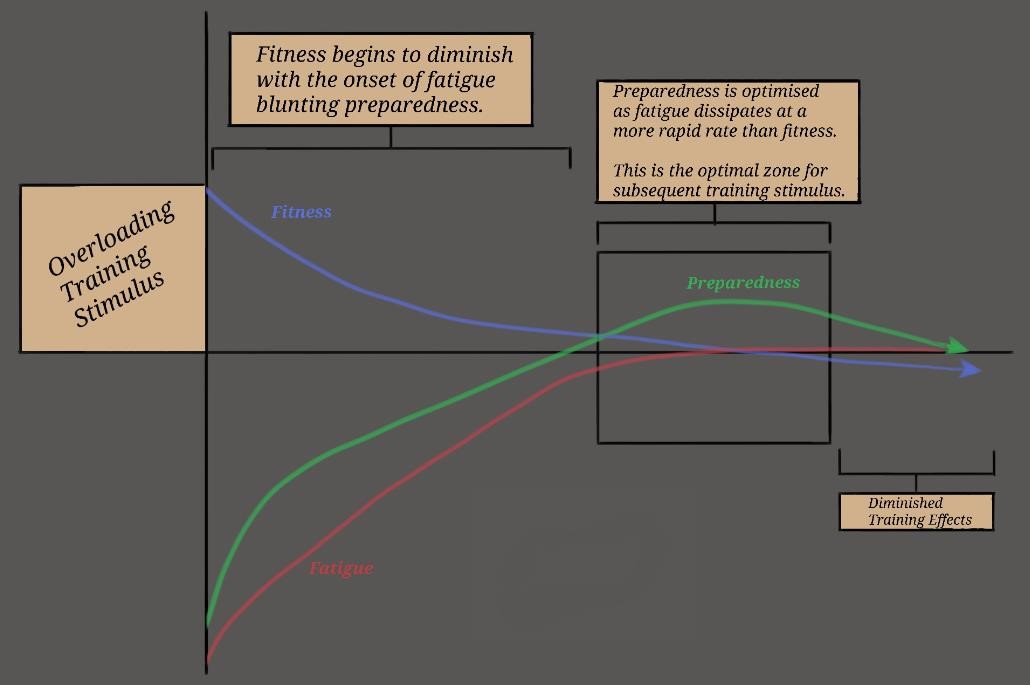
Figure 1: The fitness fatigue model (Chiu and Barnes, 2003; Plisk and Stone, 2003; Stone, Stone and Sands, 2007) adapted from Haff and Triplett (2015).
The key physiological principle that underpins the optimisation of performance is the fitnessfatigue relationship
Figure 1) (Chiu and Barnes, 2003; Plisk and Stone, 2003; Stone, Stone and Sands, 2007). This essentially describes how a training strategy that minimises fatigue accumulation while also maximising adaptations will have the greatest transfer to optimal performance. This relationship precedes the delayed training effects paradigm (Figure 2) (Stone, Stone and Sands, 2007; Mujika, 2010), which aims to explain the association between the fitness-fatigue model and the supercompensation of performance (Bompa and Haff, 2009).
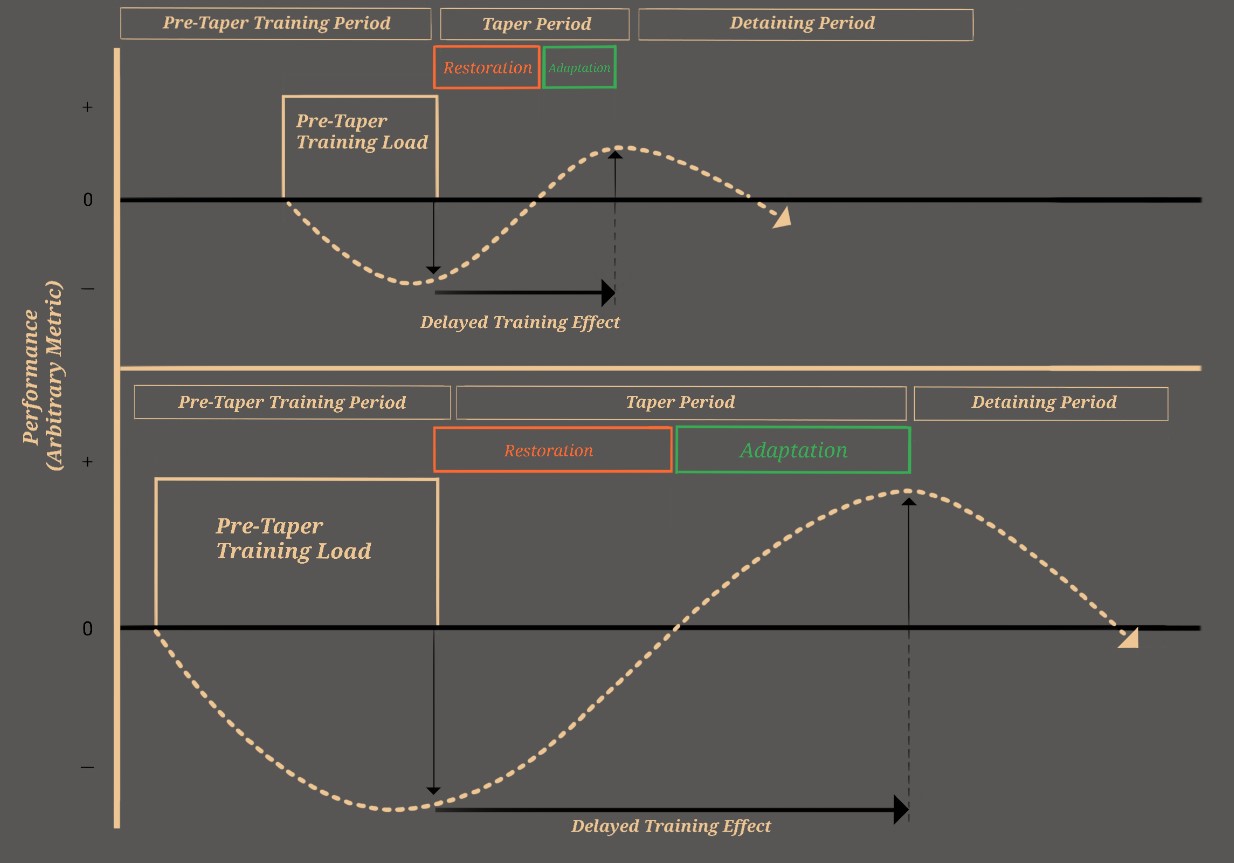
Figure 2: Delayed training effects (Mujika, 2010; Stone, Stone and Sands, 2007) adapted from (Haff, 2014).
The proposed supercompensation and adaptations of a taper above what can be achieve by continuing normal training makes it an essential tool that can be used to reach peak performance (Wilson and Wilson, 2008; Le Meur, Hausswirth and Mujika, 2012; Bosquet et al., 2007; Mujika and Padilla, 2003). Once administered correctly, the range of performance improvement from a taper ranges from 0.5% – 12% for both endurance and strength and power sports (Bosquet et al., 2007; Mujika, 2009; Mujika et al., 2004; Mujika and Padilla, 2003; Chtourou et al., 2012; Bompa and Haff, 2009; Brannstrom, Rova and Yu, 2013; Pritchard et al., 2015). Although these results are relative to the participants of each study, these improvements may have important implications for elite athletes (Hopkins, Hawley and Burke, 1999). As the aim of a taper is to dissipate accumulated fatigue and super-compensate to achieve peak performance, it is imperative to understand the physiology of how this peak performance is achieved. A full list of the proposed physiological alterations are shown in Table 1 (Luden et al., 2010; Mujika, 2009) and will be further outlined below.
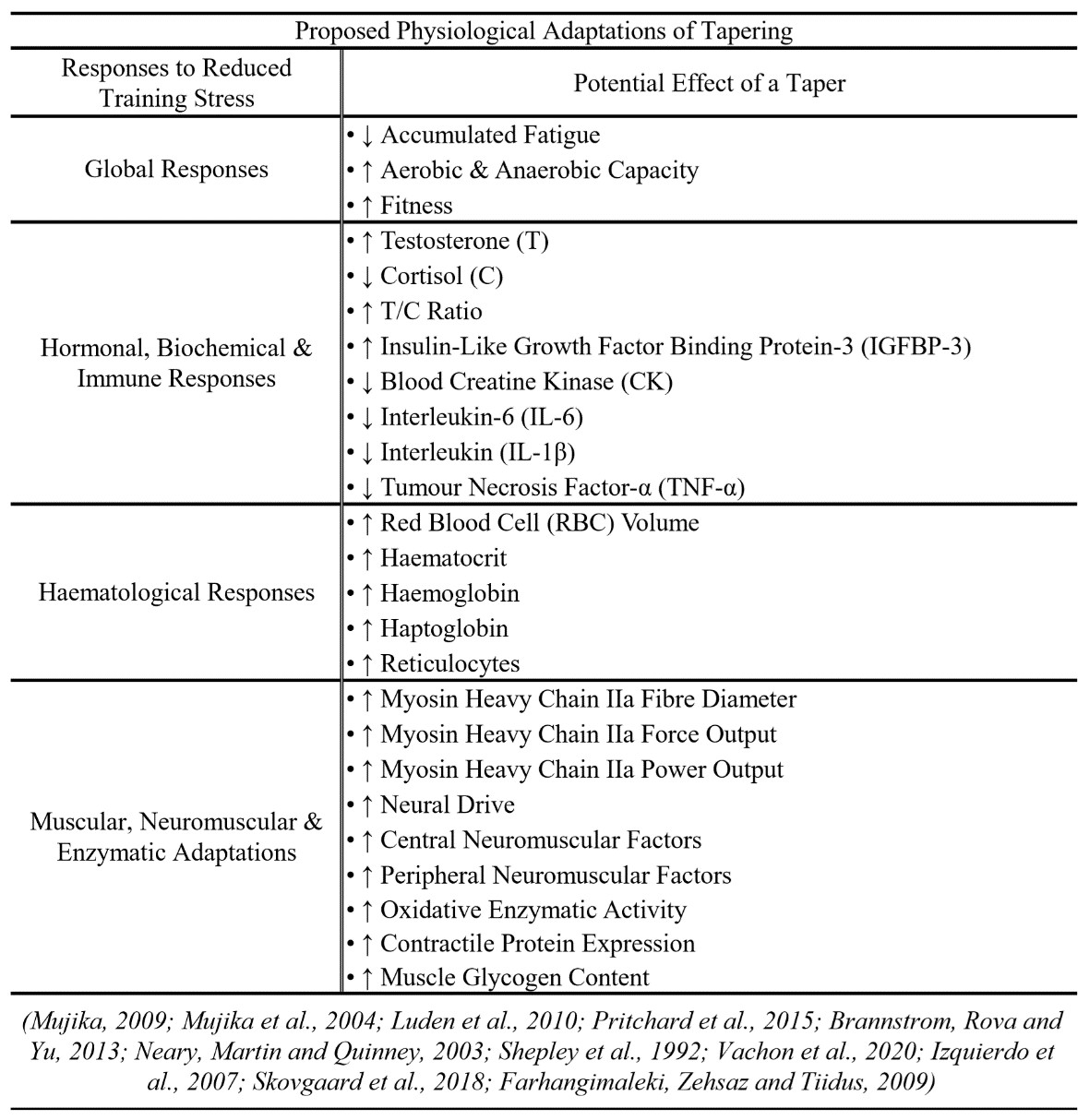
Table 1: Proposed physiological adaptations to tapering.
Physiological Adaptations to Tapering
Haematological Adaptations
One important determinant of performance that has been of focus in tapering research is aerobic capacity (VO2max) (Vachon et al., 2020; Buchheit and Laursen, 2013; Joyner and Coyle, 2008). The effect of tapering on VO2max is commonly found to either have no-detriment or elicit an increase (~1-9%) (Vachon et al., 2020; Mujika et al., 2004; Zarkadas, Carter and Banister, 1995; Mujika, 2009; Bosquet et al., 2007; Mujika and Padilla, 2003) which result in an enhancement in oxygen uptake, delivery and utilization during exercise (Vachon et al., 2020; Costa et al., 2019; Zarkadas, Carter and Banister, 1995) and has important implications for elite athletes. One of the primary cause of these changes in VO2max are the haematological changes that occur due to tapering. The planned periods of intensive training overload results in negative haematological changes including reduced haematocrit resulting from a decrease in circulating red blood cells (RBC) and haemoglobin content (Borges et al., 2012; Pizza et al., 1997; Shaskey and Green, 2000). These negative alterations are thought to be as a result of increased plasma volume, greater haemolysis and possible iron deficiency induced by training stress which causes haemodilution and hypervolaemia (Hallberg, Magnusson and Hallberg, 1984; Kaiser, Janssen and van Wersch, 1989; Weight, 1993). Elevated plasma renin activity and vasopressin concentrations during intense exercise coupled with the continuing increases in blood water-binding capacity which may also contribute to the hypervolaemia (Pittman, 2011; Mujika, 1998; Convertino, Keil and Greenleaf, 1983). These negative training-induced changes in blood content have shown to be reduced and super-compensated after a taper (Shepley et al., 1992; Mujika et al., 2004).
After a tapering period, literature has consistently demonstrated increases in total blood volume, which consisted of increases in RBC, haemoglobin content and haematocrit (Shepley et al., 1992; Margaritis et al., 2003; Mujika et al., 2000; Rushall and Busch, 1980) which can be attributed …









Responses